This article is based on 9 peer-reviewed studies from PubMed. Last updated: March 2026.
Table of Contents
INTRODUCTION
Cystolitholapaxy complications, though infrequent, range from minor postoperative discomfort to rare but serious events such as bladder perforation and urethral stricture.
This guide explores the potential complications associated with cystolitholapaxy, primarily focusing on the percutaneous cystolitholapaxy (PCCL) approach and its comparisons with transurethral and open surgical methods. While cystolitholapaxy is generally safe and effective, understanding the risks is essential for informed decision-making and optimal postoperative care.
1. Overview of Cystolitholapaxy Complications
Complication rates vary significantly based on the surgical approach and the patient’s underlying anatomy. In a single-surgeon series of PCCL for complex lower urinary tract cases, the complication rate was reported at approximately 28%, with most being minor. In pediatric populations, endourological approaches (both transurethral and percutaneous) have been associated with a complication rate of approximately 7.4% to 15%. Despite these risks, endourological management generally offers shorter hospital stays compared to traditional open surgery.
2. Intraoperative complications
Intraoperative events are relatively uncommon but require immediate recognition:
- Bladder Perforation: This is rare but may occur due to accidental loss of control of the lithotripter or during tract dilation. Perforation is more likely in patients with chronic bladder outlet obstruction and significant bladder wall thickening (trabeculation). Intraperitoneal perforation usually necessitates open surgical repair.
- Hemorrhage: Uncontrolled bleeding is considered the most common serious complication requiring active management. Bleeding can arise from urothelial injury during stone fragmentation or from the percutaneous access tract itself.
- Bowel and Rectal Injury: There is a rare risk of bowel injury during percutaneous access, particularly in patients with a history of complex abdominal surgery where bowel may be interposed in front of the bladder. Rectal injury is also a known, albeit rare, risk if control of the lithotripter is lost at the posterior bladder wall.
3. Early postoperative complications
Shortly after surgery, patients may experience the following:
- Urinary Tract Infection (UTI) and Sepsis: While post-procedural UTIs are treated with culture-directed antibiotics, septic infections are infrequent but serious, requiring fluid resuscitation and broad-spectrum antibiotics.
- Urinary Leakage: Persistent leakage of urine from the suprapubic puncture site is a common complication of the percutaneous approach. This is typically managed by maintaining a transurethral catheter for a few extra days to allow the fistula to close.
- Hematuria: Mild, self-limiting blood in the urine is common and usually resolves within 12 to 24 hours with adequate hydration.
Read: Cystolitholapaxy Recovery Time: Hospital Stay, Catheter Removal & Return to Activity
4. Late complications
Long-term risks associated with bladder stone surgery include:
- Urethral Stricture: This is a primary concern with the transurethral approach, especially in male children, due to the small caliber of the penile urethra and potential trauma from large-bore rigid instruments.
- Stone Recurrence: Patients with reconstructed bladders have a high recurrence rate, reaching up to 44%. In populations with Exstrophy–Epispadias Complex (EEC), recurrence rates are comparable between surgical approaches and are often driven by factors like mucus production and incomplete emptying.
- Fistula Formation: Vesicocutaneous fistulas (abnormal tracts between the bladder and skin) are significantly more common in EEC patients following open surgery (up to 45.45%) compared to percutaneous approaches, which have shown zero incidence in some series.
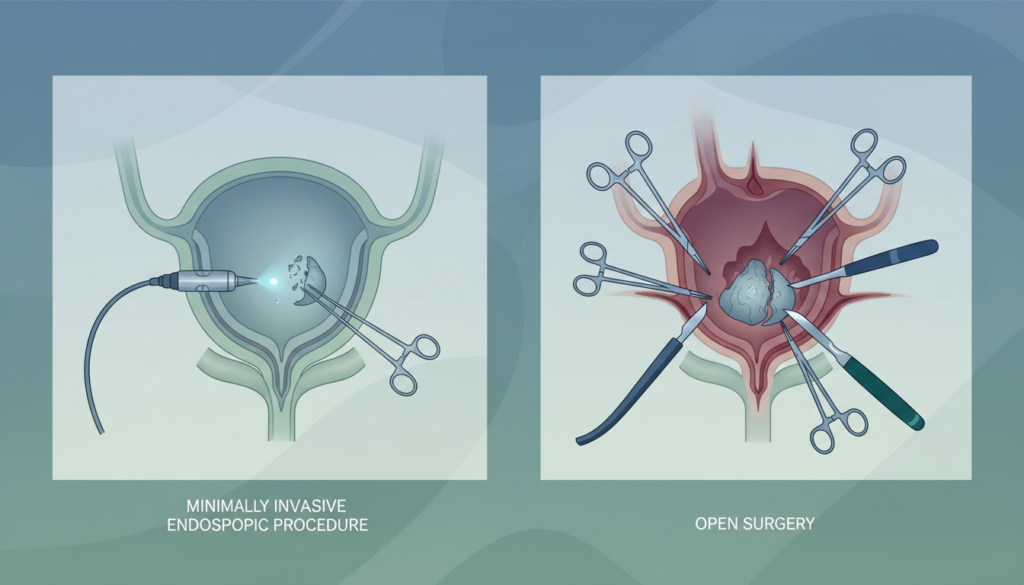
5. Complications by approach: Transurethral vs. Percutaneous
- Transurethral (TUCL): Associated with a higher risk of urethral trauma and subsequent stricture formation. For large stones, TUCL can be more time-consuming as fragments must be small enough to pass through the urethra.
- Percutaneous (PCCL): Offers a direct trajectory for large-bore instruments, reducing the risk of urethral injury. However, it introduces risks specific to abdominal access, such as suprapubic site leakage and potential injury to adjacent abdominal organs.
6. Complications in special populations
- Pediatric Patients: These patients are at a higher risk for urethral complications. PCCL is often preferred for stones >1 cm to protect the delicate pediatric urethra.
- Reconstructed/Augmented Bladders: Access is more complicated due to the risk of injury to the mesentery or the reconstructed bowel segment. These patients require longer postoperative catheterization to allow the reservoir to heal.
- Exstrophy–Epispadias Complex (EEC): This population has attenuated fascia and is highly vulnerable to mucosal violations, making minimally invasive percutaneous approaches safer for avoiding postoperative fistulas compared to open surgery.
7. Clavien-Dindo grading of complications
Medical literature uses the Clavien-Dindo system to standardize the reporting of surgical complications:
- Grade I: Minor complications like transient fever or self-limited hematuria.
- Grade II: Complications requiring pharmacological treatment, such as a fever >38°C treated with antibiotics.
- Grade III: Complications requiring surgical, endoscopic, or radiological intervention, such as ongoing hemorrhage necessitating operative clot evacuation.
Read: What is Cystolitholapaxy?
8. How to minimize complication risk
- Preoperative Imaging: Utilizing CT scans helps define the anatomy and ensure a safe percutaneous access window, particularly to avoid bowel injury.
- Direct Vision Guidance: Performing the percutaneous puncture under cystoscopic or ultrasound guidance significantly reduces the risk of injuring the posterior bladder wall or the rectum.
- Infection Control: Administering prophylactic antibiotics within one hour of the procedure is standard practice.
- Recurrence Prevention: Regular bladder irrigations with saline are instructed for patients with reconstructed bladders to evacuate debris and reduce stone recurrence.
9. When to seek immediate medical attention
Patients should contact their surgical team immediately if they experience any of the following warning signs:
- Significant Bleeding: Heavy blood in the urine or through the suprapubic tract.
- High Fever: A temperature >38°C which may indicate a UTI or sepsis.
- Acute Abdominal Pain or Distention: This can be a sign of a missed bladder perforation or leakage of irrigation fluid into the abdominal cavity.
- Persistent Leakage: Continual urine leakage from the skin incision site after the catheter is removed.
REFERENCES
- Ali, M., Hashem, A., Helmy, T. E., Zewin, T., Sheir, K. Z., & Shokeir, A. A. (2019). Shock wave lithotripsy versus endoscopic cystolitholapaxy in the management of patients presenting with calcular acute urinary retention: A randomised controlled trial. World Journal of Urology, 37, 879–884.
- Al-Marhoon, M. S., Sarhan, O. M., Awad, B. A., Helmy, T., Ghali, A., & Dawaba, M. S. (2009). Comparison of endourological and open cystolithotomy in the management of bladder stones in children. The Journal of Urology, 181(6), 2684–2688.
- Almesned, R. K., Binjawhar, A., Altaweel, W., & Alomar, M. (2025). Percutaneous cystolitholapaxy in reconstructed bladder through the bowel segment. Urology Annals, 17(1), 64–67.
- Gamal, W., Eldahshoury, M., Hussein, M., & Hammady, A. (2013). Cystoscopically guided percutaneous suprapubic cystolitholapaxy in children. International Urology and Nephrology, 45(4), 933–937.
- Lee, M. S., Sledge, T. R., Seyer, A. K., Qi, R., & Koo, K. (2025). How I do it: Percutaneous cystolitholapaxy for bladder stones with complex lower urinary tract anatomy. Canadian Journal of Urology, 32(4), 325–333.
- Mahran, M. R., & Dawaba, M. S. (2000). Cystolitholapaxy versus cystolithotomy in children. Journal of Endourology, 14(5), 423–426.
- Metwally, A. H., Sherief, M. H., & Elkoushy, M. A. (2016). Safety and efficacy of cystoscopically guided percutaneous suprapubic cystolitholapaxy without fluoroscopic guidance. Arab Journal of Urology, 14(3), 211–215.
- Wollin, T. A., Singal, R. K., Whelan, T., Dicecco, R., Razvi, H. A., & Denstedt, J. D. (1999). Percutaneous suprapubic cystolithotripsy for treatment of large bladder calculi. Journal of Endourology, 13(10), 739–744.
- Yang, J., Heap, D., Maxon, V., Robey, C., Maruf, M., Michel, C., Di Carlo, H. N., Gearhart, J. P., & Crigger, C. B. (2025). Percutaneous cystolitholapaxy and open cystolithotomy in exstrophy–epispadias complex: A comparative approach to bladder stone management. Journal of Endourology, 39(11), 1172–1180.