This article is based on 3 peer-reviewed studies fromPubMed. Last updated: March 2026.
Table of Contents
1. Introduction
Cystolitholapaxy vs lithotripsy — choosing between these two bladder stone treatments can significantly impact your recovery time, success rate, and overall outcome. This evidence-based guide breaks down every key difference to help patients and clinicians make the right decision.
Cystolitholapaxy is an endourological procedure that involves both the fragmentation of bladder stones and their immediate, active removal from the bladder. The term is derived from the Greek lithos (stone) and lapaxis (evacuation). In contrast, lithotripsy strictly refers to the act of crushing or fragmenting the stone into smaller pieces. In the context of bladder stones, lithotripsy can be performed extracorporeally (from outside the body) or intracorporeally (within the bladder during an endoscopic procedure).
Clinicians and patients must understand the difference because while lithotripsy may break a stone, it does not always guarantee the clearance of fragments. Cystolitholapaxy aims for a “stone-free” state in a single session by ensuring that no debris is left behind to cause further obstruction or serve as a nidus for new stone formation.
——————————————————————————–
2. What is Cystolitholapaxy?
Cystolitholapaxy is defined by its two-stage mechanism: fragmentation followed by active evacuation.
- Mechanism of Action: The surgeon accesses the bladder through an existing orifice (transurethral) or a surgically created tract (percutaneous). Once the stone is visualized, it is stabilized and then broken down using various energy sources.
- Fragmentation and Removal: Modern systems, such as the AH-1 Stone Removal System (SRS), utilize a specialized jaw to grasp and fix stones in place, preventing them from “rolling” in the large bladder cavity during treatment. This stabilization allows for more efficient delivery of energy (such as holmium laser or pneumatic probes). Once fragmented, the SRS or similar devices automatically collect and wash out fragments synchronously through an outer sheath.
- Types of Access:
- Transurethral Cystolitholapaxy (TUCL): The most common approach, where instruments are passed through the urethra. While effective, it can be limited by urethral caliber, particularly in male children or patients with strictures.
- Percutaneous Cystolitholapaxy (PCCL): Access is gained through a small suprapubic incision into the bladder. This mirrors the framework of percutaneous nephrolithotomy (PCNL) used for kidney stones.
Read: Cystolitholapaxy Recovery Time: Hospital Stay, Catheter Removal & Return to Activity
——————————————————————————–
3. What is Lithotripsy?
Lithotripsy is primarily focused on the mechanical reduction of stone size to allow for either spontaneous passage or easier extraction.
- Mechanism of Action: Lithotripsy utilizes high-energy waves to disrupt the crystalline structure of the stone.
- Types:
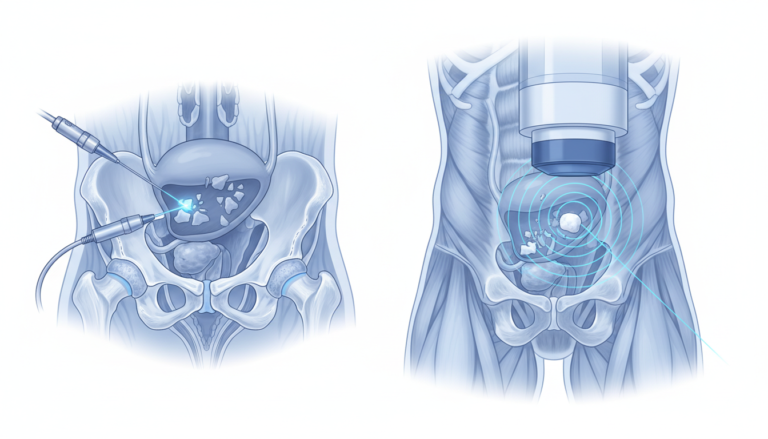
- Extracorporeal Shock Wave Lithotripsy (SWL/ESWL): A non-invasive method using shock waves generated outside the body. While popular for kidney stones, its use in bladder stones is often limited by the presence of bladder outlet obstruction, which prevents fragments from passing spontaneously.
- Intracorporeal Lithotripsy: Performed during an endoscopic procedure. Common energy modalities include pneumatic (ballistic) energy, which works like a miniature jackhammer; ultrasonic energy, which vibrates at high frequencies to emulsify the stone; and holmium laser, which vaporizes stone tissue. Some advanced devices combine these energies (ballistic + ultrasonic) with suction to facilitate simultaneous fragmentation and evacuation.

4. Head-to-Head Comparison
Clinical studies comparing different endoscopic techniques provide specific data on their efficacy and safety:
| Feature | Cystolitholapaxy (SRS/Advanced) | Transurethral Lithotripsy (Cystoscope) | Percutaneous (PCCL) |
|---|---|---|---|
| Stone-Free Rate | 100% | 100% | 96% – 100% |
| Operative Time | 5.5 – 49.3 min (size dependent) | 69.2 ± 16.3 min | 46 ± 7.3 min |
| Hospital Stay | < 48 hours (standard) | 1.3 ± 0.4 days | 2.1 ± 0.15 days |
| Complications | Low; avoids urethral entries | Urethral injury risk (multiple entries) | Suprapubic tube morbidity |
Operative time is significantly influenced by the instrument used. A transurethral nephroscope is often faster (32.1 min) than a standard cystoscope (69.2 min) because the wider lumen of the nephroscope allows for the passage of larger fragments. When using advanced systems like the SRS for single stones, times can be as low as 5.5 minutes for stones <2 cm.
——————————————————————————–
5. When is Cystolitholapaxy Preferred?
Cystolitholapaxy is the preferred clinical choice in several scenarios where stone clearance is the primary goal:
- Large Stone Burden: For multi-centimeter stones, cystolitholapaxy (especially via a percutaneous route) provides a direct trajectory and allows for the use of large-bore instruments (24–30 Fr) that can evacuate large fragments quickly.
- Complex Anatomy: PCCL is preferred when transurethral access is infeasible, such as in patients with a closed bladder neck, severe urethral stricture disease, or those with a continent catheterizable channel that must be protected from mechanical trauma.
- Failed Lithotripsy: If a patient has previously undergone SWL but was unable to pass the fragments due to poor bladder emptying or large residual gravel, an active evacuation (cystolitholapaxy) is required.
Read: What is Cystolitholapaxy?
6. When is Lithotripsy Preferred?
Pure lithotripsy (particularly ESWL) or less aggressive fragmentation is sometimes chosen based on specific patient factors:
- Ideal Stone Characteristics: Smaller, solitary stones in a patient with a wide-caliber urethra and no bladder outlet obstruction are the best candidates for simple fragmentation.
- Patient Preference and Fitness: SWL may be attractive to patients who wish to avoid anesthesia or an invasive surgical incision.
- Contraindications to Cystolitholapaxy: Percutaneous access may be contraindicated in patients with a history of recurrent bladder malignancy or those with pelvic prosthetic devices, such as an artificial urinary sphincter or penile implant reservoir, which could be damaged during tract creation.
——————————————————————————–
7. Special Populations
- Pediatric Patients: The small caliber of the pediatric urethra makes transurethral procedures risky, with a higher chance of iatrogenic urethral stricture formation. For stones >1 cm, percutaneous approaches are often safer for protecting the delicate urethra.
- Elderly Patients: Bladder stones in older men are frequently secondary to Benign Prostatic Hyperplasia (BPH). Advanced cystolitholapaxy systems can be combined with Transurethral Resection of the Prostate (TURP) in a single session, effectively treating the stone and its underlying cause simultaneously.
- Reconstructed Bladders: Patients with bladder augmentations using bowel segments are at high risk for stones due to mucus production and urinary stasis. PCCL through the bowel segment is a reliable and safe approach that avoids damaging continent stomas.
——————————————————————————–
8. Clinical Recommendations
The current evidence supports a tailored approach to bladder stone management:
- For Small Stones (<2 cm): Transurethral cystolitholapaxy using a nephroscope or a specialized removal system (SRS) is safe, efficient, and offers the shortest hospital stay.
- For Large or Multiple Stones: Percutaneous cystolitholapaxy (PCCL) should be considered to minimize operative time and reduce the number of urethral entries, thereby decreasing the risk of strictures.
- For Complex Anatomy: PCCL is the gold standard for protecting reconstructed urinary tracts or continent channels.
——————————————————————————–
9. Conclusion
The management of bladder stones has evolved into a highly specialized field of endourology. While simple lithotripsy serves the purpose of breaking down a stone, cystolitholapaxy represents a more complete surgical solution by ensuring the stone is fragmented and entirely evacuated.
Key Takeaways:
- Efficacy: Both methods have high stone-free rates, but cystolitholapaxy is more efficient for large stone burdens.
- Safety: Percutaneous access (PCCL) is a critical tool for patients with complex anatomy or pediatric patients to avoid urethral injury.
- Innovation: New devices that combine stabilization, fragmentation, and suction are setting new standards for reducing operative time.
Future directions in bladder stone treatment involve further refinement of “mini-PCCL” instruments and the integration of single-port surgical techniques to continue reducing procedural morbidity.
REFERENCES
- Lee, M. S., Sledge, T. R., Seyer, A. K., Qi, R., & Koo, K. (2025). How I do it: Percutaneous cystolitholapaxy for bladder stones with complex lower urinary tract anatomy. Canadian Journal of Urology, 32(4), 325–333. https://pubmed.ncbi.nlm.nih.gov/40910330/
- Li, A., Ji, C., Wang, H., Lang, G., Lu, H., Liu, S., Li, W., Zhang, B., & Fang, W. (2015). Transurethral cystolitholapaxy with the AH-1 stone removal system for the treatment of bladder stones of variable size. BMC Urology, 15(9). https://pmc.ncbi.nlm.nih.gov/articles/PMC4343269/
- Singh, K. J., & Kaur, J. (2011). Comparison of three different endoscopic techniques in management of bladder calculi. Indian Journal of Urology, 27(1), 10–13. https://pubmed.ncbi.nlm.nih.gov/21716932/